
The Goldilocks challenge – too much, too little, or not enough…or is it just right?

How ‘bad’ do you need to be to gain a diagnosis, and if you are not ‘bad enough’ what does that really mean? What does ‘just right’ really mean? Is this if you fit into a rigid diagnostic framework or a specific service model?

OR is it my role to consider what is just and right for you?
The ‘Goldilocks challenge’ is one we often see. This is the fact that you only gain a diagnosis if you are ‘bad enough’ in one specific cognitive domain for example, if we consider some conditions relating to neurodiversity. For example, you need to have significant challenges with reading, spelling or writing to an agreed level on a specific test or tests to get a diagnosis of Dyslexia. If you score just below a specific diagnostic threshold (which may vary from country to country and even area to area) then you are not dyslexic(!). This is despite still having the challenges. How does this dichotomous decision-making help you as a person?
So this made me think about the question several people have asked me this week:
‘Do you think it’s a good thing to gain a diagnosis?’
It made me think about my role as a doctor and my experiences running a clinical center for more than 20 years and also what I do now as a CEO of Do-IT Solutions and the rationale for the development of the Do-IT Profiler system. This is a modular accessible tool that provides a means of gathering information to help support the person/child in the context of their lives.
I often have lots of discussions with people about moving away from medical models towards more social models of practice. At the same time, I have lots of people still wanting a diagnosis for a specific condition. A Goldilocks dilemma!
For children and young people
The reality is receiving an accurate and timely diagnosis can be beneficial to children with neurodevelopmental disorders (NDDs) and their caregivers. Accurate early diagnoses can prevent the development of associated comorbidities (and secondary impact of others failing to see your strengths leading to lowered self-esteem and lost confidence). Most importantly a diagnosis sadly can be the only way to ensure access to appropriate early intervention services – during a period of active neuroplasticity.
Specifying needs can lead to children with speech and language delay benefiting from a focused intervention that can impact their ability to socially interact, make friends, and become literate. Understanding specific movement difficulties (Developmental Coordination Disorder( also known as Dyspraxia) can help to decide that handwriting for example is painful for that child and provide appropriate guidance about assistive technology.
Neurodiversity and Resilience – ‘catch-up’ …. ‘bounce-back…what does this mean for some?
In adults
Gaining a diagnosis can be a revelation and can make sense of failings, misunderstandings, and frustrations over many many years. See the recently published story: https://www.thetimes.co.uk/article/i-was-diagnosed-with-adhd-at-37-this-is-my-story-jqs77jl6h?utm_medium=Social&utm_source=Twitter#Echobox=1617961033
I was talking with someone in the past few weeks who described starting and stopping jobs, impulsively acting in situations, and resulting in getting in trouble with the police as a young person. They had also fallen out of several close relationships. They talked of the joy today of being understood by those close to them and understanding themselves better. The diagnosis (initially rejected by them) became a new beginning. It has also resulted in taking medication for ADHD which now means they have excelled at work and have a stable wonderful relationship. They also share their story with others and help them to know it is safe to be different and diverse.

A perspective has been gained on why society has to change and that past challenges were about not fitting into a rigid system that was not ‘just right for them.
So diagnosis – is it good or bad?
The question on the surface seems relatively simple to answer. In a perfect world, I may say yes if it really was the magical key to opening doors to opportunity and lowering barriers to success. But it really depends on how the diagnosis is given and what information is gathered in the process. It should not be a tick box exercise otherwise we end up drawing the wrong conclusions from missing pieces of people’s lives. No one should be diagnosed with ADHD or Autism in 20 minutes!
So how do I respond to this question in a meaningful way?
We need to start by saying why here, why now, and what for?
· Needing to gain a diagnosis – access resources, a ticket to gain entry into a support system, a financial value?
· Wanting to gain a diagnosis – taking meaning from it, wanting a language to use with others, obtaining an identity that fits you?
· Why now– important to understand the past and not keeping the same mistakes over and over again; understanding what is the right setting( e.g. for work) for yourself?
You may feel elated if you get the diagnosis you think you may have. At the same time, a label given to you by a diagnostician may not be the magic wand that you expected. It may not answer all your questions. It may not make sense if it is rushed or considered in silos.
There may be a sense of disappointment when it doesn’t necessarily come with all the answers to some functional or practical concerns that you may have.
· Which diagnosis? Do you have a preconceived idea of the diagnosis you want? Remember that ADHD/ASC/Dyslexia/DCD(Dyspraxia)/Dyscalculia all often co-occur with other conditions including anxiety, depression, epilepsy for example.
· Will the person(s) consider the whole picture or just a slice of you? Do you understand that an assessment may only look at parts of you/your child depending on the professional you see and their range of expertise? e.g. an educational psychologist may not assess for ADHD, Developmental Language Disorder, or Autism Spectrum Condition but may focus more on Dyslexia despite them often co-occurring. That’s why it is so important to take a person-centered approach to diagnosis.
· Would you prefer to only get one diagnosis and prefer that the diagnostician does not consider other diagnoses that may commonly overlap, for example, with ADHD which can co-occur with mood disorders, anxiety, conduct disorder, and substance use disorder, obsessive-compulsive, personality disorder, passive-aggressive personality disorder, depressive personality disorder, narcissistic personality disorder, and borderline personality disorder (BPD).
· The diagnostician will also need to consider the differential diagnosis to ensure they draw the appropriate conclusions. For example, when considering a diagnosis of Dyspraxia /Developmental Coordination Disorder also checking out Cerebral Palsy or Hypermobility Ehlers Danlos Syndrome (HEDs?) or Parkinson’s or other reasons for motor challenges.
· How will you feel if the diagnostician says you don’t have the diagnosis you suspected and tell you it’s something else?
· What happens if you end up with several diagnoses – which ones will you tell others about – all or some? ( What do you think employers think at an interview if you say you have ADHD/Dyspraxia and Dyslexia ( all often overlap)? Will you choose to tell them about all or some of the diagnoses?)
The diagnosis you may get or want maybe:
· Dependent on whom you see
· How good the person(s) is listening to you and taking a ‘history’ to gain a complete picture

“A smart mother makes often a better diagnosis than a poor doctor.”
— August Bier
· Dependent on the time spent
· What is available in your area
· The only one you can afford
· The service with the lowest waiting lists
· The one that is more acceptable to you
· The one that provides more resources e.g. Autism ‘trumps’ Developmental Language Disorder in gaining speech and language intervention irrespective of the degree of impact.
· The one that others have heard of
· The one that professionals have had training in
· A representation of part of you and doesn’t actually consider other elements that co-occur
· The wrong one because of misconceptions about gender, context, culture, or gained as a result of missing crucial information
· Dependent on your ability to be heard and listened to
“An observant parent’s evidence may be disproved but should never be ignored.”
— Anonymous, Lancet (1951), 1, 688
As a medical doctor, I spend a lot of time thinking about what is my role as a diagnostician? I think it important to have someone acting in a detective role, sifting and collating the information, and making sense of the different symptoms and signs, strengths, and challenges in that person’s life. Taking a comprehensive history and considering how they all fit together. Without a process of undertaking a differential diagnosis and considering what else could the symptoms, signs, strengths, and challenges that are presented to us we have the risk of coming to false conclusions. This can have a real impact on people’s lives.
Our training, working best when working with others in an interdisciplinary manner. This doesn’t always happen and we too often work in silos. But there is a growing understanding of recognizing the need to take a more person-centered approach to assessment to stop people running around, costing a lot in time, money but most of all angst. Siloed practices don’t ever achieve a person-centered profile being ascertained. They can cause confusion and misunderstanding. They can also cost a lot!
Is the alternative to others diagnosing is a DIY approach? The challenge is when we make a checklist of traits we may try to fit ourselves into the shape that we want to fit into based on our current understanding and may miss out on vital information. Some of the signs and symptoms of Developmental Coordination Disorder ( also known as Dyspraxia) could be symptoms of Cerebral Palsy, even Parkinson’s, or a brain tumor! Some of the signs and symptoms of ADHD can be similar to Traumatic Brain Injury. Some of the signs and symptoms of Developmental Language Disorder can be misconstrued as ‘behavior’ or social and emotional difficulties in children. If we self-diagnose we may end up missing other important and treatable conditions such as nocturnal epilepsy or genetic conditions such as Neurofibromatosis 1.
So is a diagnosis essential?
Probably not for all. But we do need some triage approaches so practical support can be given if there are ‘red flags’ a diagnosis ascertained if appropriate. Recognising, for example, a child has signs of epilepsy may be important to treat that epilepsy. Considering symptoms of depression may be important in someone on the Autistic Spectrum.
“Diagnosis is not the end, but the beginning of practice.”
— Martin H. Fischer; Fischerisms (1944)
I think the Goldilocks dilemma – is in fact all about being ‘just right for you. It’s not about espousing the social model and chucking out the medical model. By taking a more dynamic and tiered approach with a more functional and practical to start is in reality is the best mixes of the social and medical models. There is growing interest in moving away from categorical approaches and using the International Classification of Functioning, Disability, and Health ((ICF) World Health Organization). The detailed framework has been developed and used for many conditions including ADHD, DCD, and Autistic Spectrum Conditions. ICF offers a comprehensive framework for understanding functioning and disability and takes a dynamic bio-psycho-social perspective. It recognizes that people change over time and also their environment and those they interact with do also.
The framework considers four interacting components :
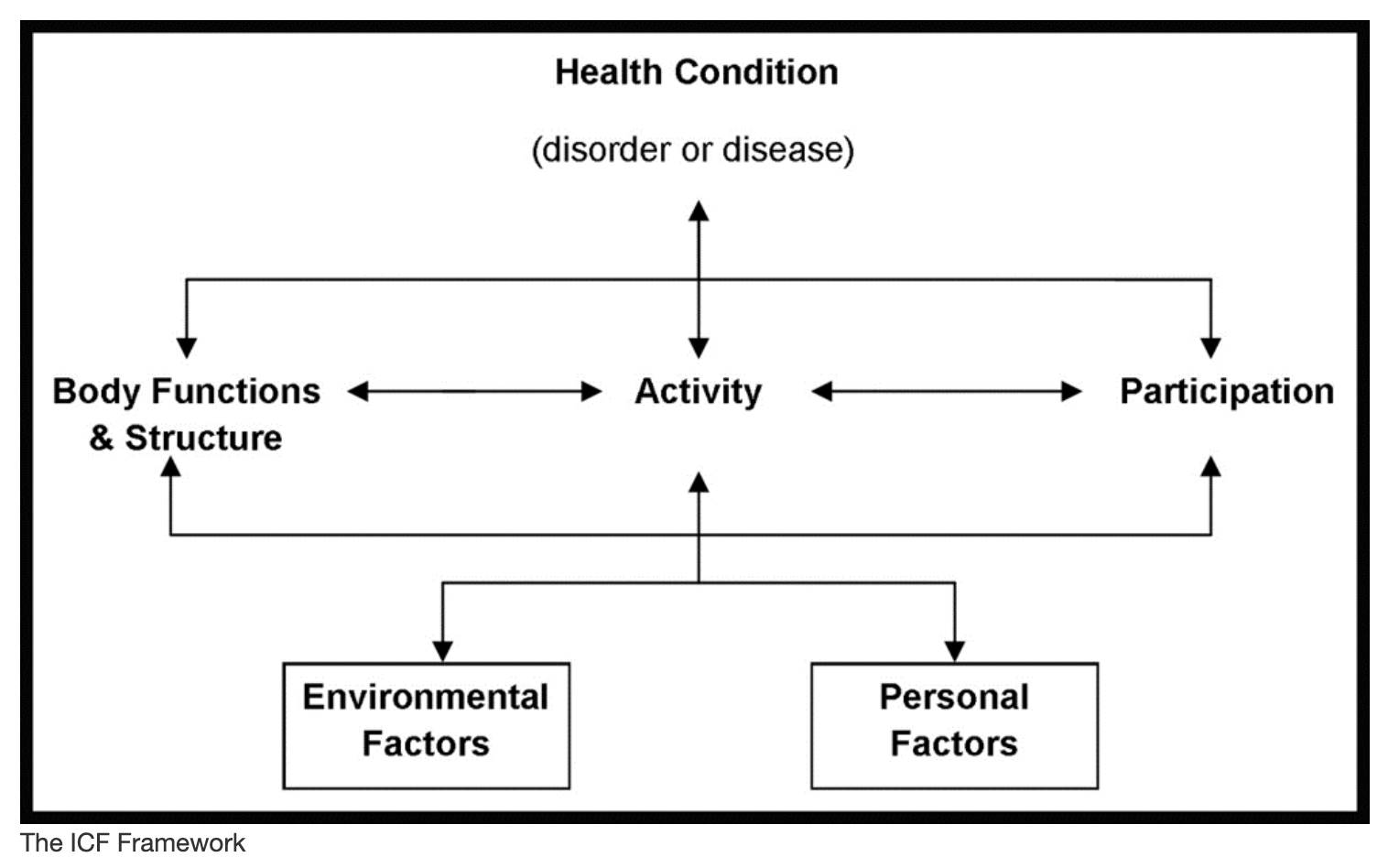
(1) body functions and structures;
(2) activities and participation;
(3) environmental factors;
(4) personal factors.
More than fifteen years ago I started developing a Do-IT Profiler as a consequence of running an interdisciplinary clinical center because of a need to understand how we can bring the parts of a person together to understand the whole in the context of their lives. Today, this system is increasingly being used in schools, apprenticeships, colleges, universities, into employment, in employment, and in all aspects of the justice system. The system varies in content and the guidance varies very importantly depending on the context. This is trying to help take a person-centered. Do-IT tools are not THE answer to a diagnosis and never will be. People with skills diagnose. But sometimes having the tools to help can make a real difference.

“For most diagnoses, all that is needed is an ounce of knowledge, an ounce of intelligence, and a pound of thoroughness.”
— Anonymous
Arabic Proverb. In Lancet (1951).
I am a parent and grandparent of a very wonderful neurodivergent family and know first- hand why being understood is very important and why getting the right diagnosis makes all the difference and the wrong one being at the least meaningless and disappointing.
I am also the CEO of Do-IT Solutions. It is a tech-for-good company trying to make a bit of a difference in this messy world we live in and help some people be their best. We have completed hundreds of thousands of assessments using the system which generates a person-centered report and practical guidance as a starting point for further discussion and exploration. It’s not magic. The system is evolving and changing as we understand more.
Contact me if you want to know more about how Do-IT can work with you.
Napomena o autorskim pravima: Dozvoljeno preuzimanje sadržaja isključivo uz navođenje linka prema stranici našeg portala sa koje je sadržaj preuzet. Stavovi izraženi u ovom tekstu autorovi su i ne odražavaju nužno uredničku politiku The Balkantimes Press.
Copyright Notice: It is allowed to download the content only by providing a link to the page of our portal from which the content was downloaded. The views expressed in this text are those of the authors and do not necessarily reflect the editorial policies of The Balkantimes Press.